


Feeding early in life, particularly for a newborn, is typically breast-feeding or a bottle of formula. Infants tend to cry when they’re hungry and stop eating when they’re full. It’s a very natural and important process that tends to have cues as to how well the baby is tolerating its diet, whether that be spit up or colic or other agitations such as gas. While newborn feeding can be route with challenges for both mom and baby it tends to be a simpatico engagement that yields good results for most babies early in life.
In utero, a developing fetus is nourished through its umbilical cord tied to the mom. The infant receives the most personalized form of nutrition, informed by biological feedback, and while some experience metabolic challenges, by and large, most fetuses achieve optimal growth, using this dyad mechanism.
Where true challenges arise is when a fetus is delivered prior to 37 weeks gestation and with increasing frequency as young as 22 weeks gestation, that is a preterm infant, and nutrition now needs to be provided from sources that are not tailor-made to her or him. This period immediately following premature delivery would have been the third trimester of pregnancy – a critical developmental epoch for a fetus.
In these cases, not only can the infant not communicate when it’s hungry, nutrition often must be delivered intravenously or via a tube to the gut as the baby cannot suck, swallow, and breathe to breast-feed or take a bottle and in many cases the organs of the gut have not completed development. This nutritional labor of love falls to the clinical care teams in the neonatal intensive care unit. Preterm infants are often fed every 2 to 3 hours – tiny amounts of nutrition that are attempting to meet their needs and match their energy expenditures. It may surprise you to know that a preterm infant needs as many calories per kilo per day as Michael Phelps when he was swimming in the Beijing Olympics when he was consuming nearly 12,000 calories a day. Preterm infants need this to meet their ‘peak performance’ to optimize brain development and growth.
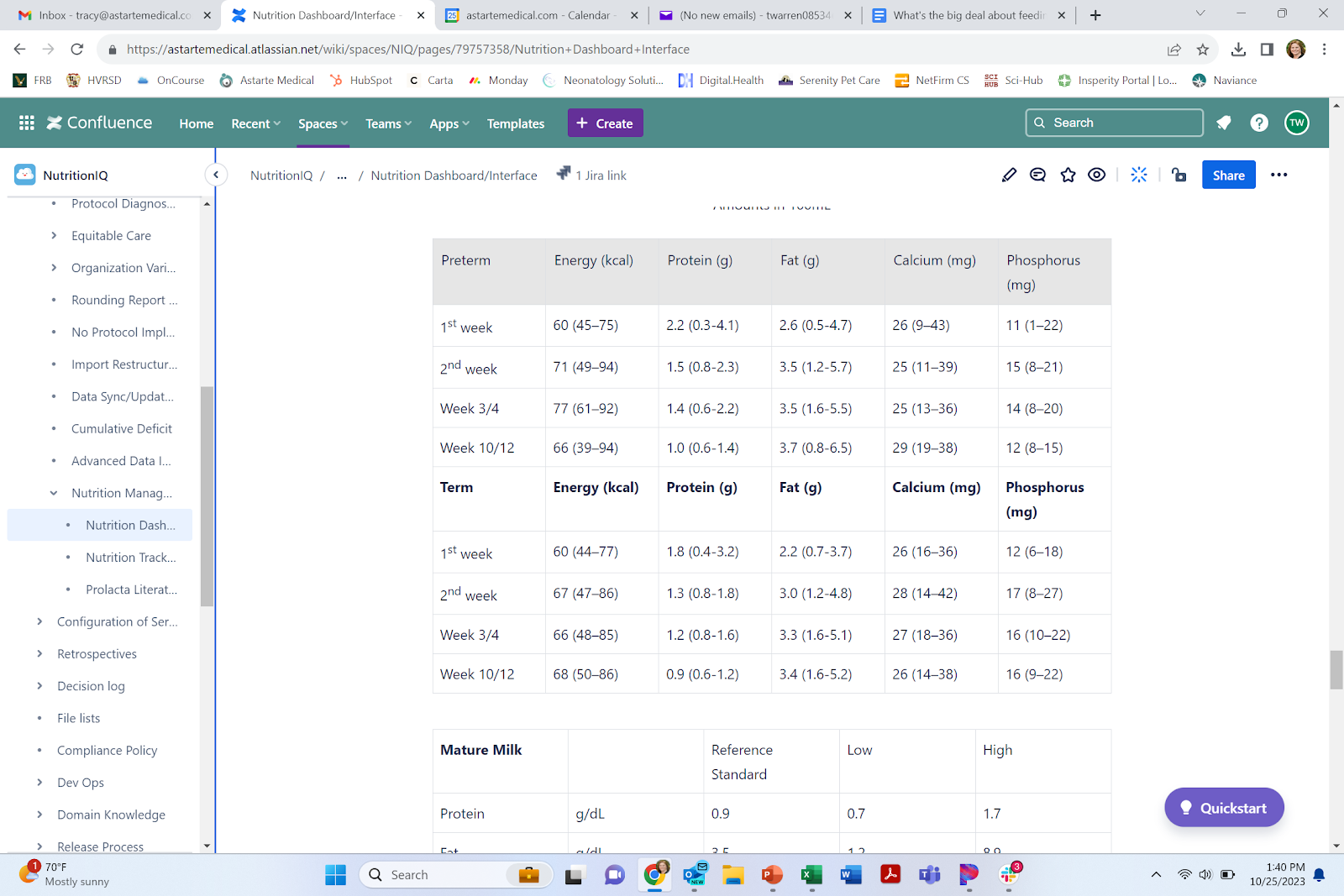
As with adults, nutrition is not simply about calories. Various components of nutrition are essential for a baby to grow and develop properly, and these elements need to be accounted for in any provision of nutrition to these vulnerable infants. Moreover, as a preterm infant matures, her nutritional targets change, exacerbating the risk of errors or omissions and increasing the complexity for clinical teams:
This table illustrates the target nutrients per kg of body weight for a typical 28-week gestation preemie. The values in “( )” represent current academically supported ranges for various babies.
Clinical teams have a relentless and dogged pursuit of achieving optimal nutrition, including the balance of proteins, lipids, carbohydrates, vitamins, and micronutrients to support growth and development that the fetus would have achieved inside mom. Not only is it mathematically challenging and labor-intensive it is fraught with fits and starts as concerns about intolerance, and G.I. disease create doubt in the minds of the clinical care teams. Physical and natural limits on the total volume and the concentration (osmolality) of the diet create the need for delicate and deliberate balancing.
Beyond an intravenous nutrition-based diet, the typical preterm infant will progress to the mother’s own milk, donor milk, or preterm infant formula. However, human milk creates an inconsistent diet with unknown macro and micronutrients, so clinical teams use reference values. This complicates the calculations for achieving optimal targets given the base diet contributions are unknown and inconsistent. Here’s an example to illustrate the complexity and calculation intensity of feeding a preterm infant.
Baby Warren is a 28-weeker (born 12 weeks early) who’s been in the NICU for two weeks, post-menstrual age of 30 weeks. Today she weighs 1300 grams. She is being fed human donor milk (mother’s unavailable – and while Mom’s milk would have matched the required nutritional profile better, Donor milk is universally from humans that are much further postpartum) and is on full enteral (no IV nutrition) feeding on a Q3 schedule (every 3 hours). The protocol recommends feeding at a rate of 120ml/kg/day at this stage in the journey.

Questions: How many mL of donor milk should Baby Warren receive at her 1pm feeding? If you are providing unfortified donor milk, does she meet each of her macronutrient targets?
Nutritional Targets (macronutrients)
Decileters (dL)
| Calories/ | Assumed in Human Milk | |||
| Component | Target Range | Gram | Term (donor) | Preterm (mom’s) |
| Total Fluid | 135-200 mL/kg/day | |||
| kcal | 110-135 kcal/kg/day | 70kcal/dL | 78kcal/dL (61-94) | |
| Protein | 3.5-4.5g/kg/day | 4kcal/g | 1.2 g/dL | 2.2g/dL |
| <28 weeks | 4g/kg/day | 1.3 – 3.3 g/dL | ||
| 28-32 weeks | 3.5g/kg/day | 1.3 – 2.5 g/dL | ||
| 32-37 weeks | 3g/kg/day | 1.2 g/dl | ||
| Fat/Lipids | 4.8-6.6g/kg/day | 9kcal/g | 3.6g/dL | 4.4g/dL (2.6 – 6.8) |
| Carbohydrates | 11.6-13.2g/kg/day | 4kcal/g | 7.4g/dL | 7.6g/dL |
Extra credit if you show your work. Solution at end of document.
While reference ranges are used for calculating these targets, in reality their compositions can vary widely among mothers and even for a given mother on a daily basis resulting in inconsistent delivery of nutrients despite clinicians’ best efforts. Deficits accumulate during the weeks and months of an infant’s stay, which causes infants to fail to reach their full potential. Nearly 50% of infants born under 32 weeks gestation experience growth faltering and nearly 40% experience neurodevelopmental delays and disabilities.
Variability In Ranges Among Human Milk
| Preterm Milk* | Term Milk | |||
|---|---|---|---|---|
| Reference | Range | Reference | Range | |
| Calories | 78kcal/dL | 61-94 | 67kcal/dL | 43-115 |
| Protein | 2.2g/dL | 1.3-3.3 | 0.9g/dL | 0.7-1.7 |
| Fat | 4.4g/dL | 2.6-6.2 | 3.5g/dL | 1.2-8.9 |
| Carbohydrates | 7.6g/dL | 6.4-8.8 | 6.7g/dL | 6-9.6 |
| * During the first 8 weeks for mothers of infants born <29 weeks gestation. |
What if, instead of reference values, one assumes the milk provided only provides the bottom end of the range when you complete the above exercise?
Probably as importantly, community hospitals or those in areas of low-resourced centers, often find themselves without resident expertise in registered dietitians or nutritionists, so not only are they caring for the sickest and tiniest infants, but the expertise is unavailable or a shared resource among the hospital. This exacerbates challenges with delivering optimal nutrition, increasing health disparities.
Knowing nutrition is the most modifiable risk factor in healthcare and recognizing the immensely challenging burden it places on clinical care teams, how can we improve infant outcomes and reduce the burden while increasing the confidence of our clinical care teams?
SOLUTION:
| 1300 | Grams | Current Weight | |||
| 120 | mL/kg/day | Total Volume Target | |||
| (1300 grams * 120 mL/kg/day)/1,000 grams /kg = 156 mL total for the day | |||||
| 156 | mL target for the day | ||||
| Q3 | Feed every 3 hours | ||||
| 24 hours in a day / 3 hours = 8 feeds per day | |||||
| 19.5 | |||||
| 156 mL total / 8 feeds = 19.5 mL per feed | |||||
| Assumed macronutrients per dL | |||||
| Kcal | 70 | kcal | |||
| Protein | 1.2 | g | |||
| Fats (lipids) | 3.6 | g | |||
| Carbohydrates | 7.4 | g | |||
| 156 mL /(100 mL/dL) = 1.56 dL per day | |||||
| Delivered Nutrients per day | |||||
| kcal | 109.2 | kcal | |||
| Protein | 1.872 | g | |||
| Fats (lipids) | 5.616 | g | |||
| Carbohydrates | 11.544 | g | |||
| Target Nutrients per kg per day | |||||
| kcal | 71 | kcal | |||
| Protein | 1.5 | g | |||
| Fats (lipids) | 3.5 | g | |||
| For Baby Warren at 1,300 grams (1.3 kg) | |||||
| Target | Delivered | variance | Surplus or deficit | ||
| kcal | 92.3 | 109.2 | 16.9 | Surplus | |
| Protein | 1.95 | 1.872 | -0.078 | Deficit | |
| Fats (lipids) | 4.55 | 5.616 | 1.066 | Surplus |
Answer if you assume low end of nutrient ranges with % variance vs. target
| Target | Delivered | variance | Surplus or deficit | % variance from Target | |
| kcal | 92.3 | 67.08 | -25.22 | Deficit | 27% |
| Protein | 1.95 | 1.092 | -0.858 | Deficit | 44% |
| Fats (lipids) | 4.55 | 1.872 | -2.678 | Deficit | 59% |
About Tracy Warren
Tracy Warren is the chief executive officer of Astarte Medical. She is a former technology startup investor who has long advocated for women’s and children’s health issues.