
When I interviewed Ronald Reagan about his health in 1980, he was 69 and poised to become the oldest person to be elected president. During our conversation, Reagan was mentally sharp. In a light moment he feigned a wrenched back and asked what I (a physician) would do for it.
I asked him about his mother’s health, and he told me that his mother had symptoms suggestive of dementia before she died. I asked what he would do if, as president, he developed the same ailment, and how he would know he had it. His doctors would follow him, he said, and he would resign if they found evidence of cognitive decline. Years later, those remarks would seem particularly noteworthy.
The interview was likely the first in which a future president and his doctors discussed the leader’s health prospectively. (That cooperation was short-lived; Reagan’s aides did not allow reporters to interview him or his doctors when he ran for re-election after what some regarded as a poor debate performance with Walter Mondale.)
For 52 years, I reported on the health of American and foreign political leaders for the New York Times, bringing my experience as a physician to what became a new journalism niche. The last presidential candidates who agreed to my interview requests were in 2004: George W. Bush (for only 10 minutes) and John F. Kerry (separate full-length conversations with Kerry and his doctor).

A question I’ve long pondered is this: How old is too old to be president of the United States?
That question is particularly relevant now, as the presumptive nominees of the two major parties in the November election will be the oldest pairing of rivals in history. President Biden is 81, and former President Donald Trump is 77. If re-elected, Biden would be 86 (the age I am now) and Trump 82 upon leaving office in 2029.
That too old question is impossible to answer, in part because our Founding Fathers did not address it. While they set an age minimum of 35 in the Constitution, there is no maximum. Maybe that is because in those early days of the republic no one could have predicted medical advances that would enable octogenarians to become presidents.
If now-standard medicines like polio vaccine and blood pressure-lowering drugs had been available to presidents like Franklin D. Roosevelt, they might have survived longer. Similarly, imagine if antibiotics were available for the assassinated James A. Garfield and William McKinley, or statins to help prevent heart attacks for Warren G. Harding and others. Better public health measures could also have helped in the 18th and 19th centuries when presidents suffered dysentery and other infections from inadequate plumbing, sewage, and sanitation in the White House and Washington swamp.
In researching the health of political leaders, I have found that sitting presidents have experienced gout, heart and circulatory ailments, cancer, phlebitis, pneumonia, Covid-19, abscesses, and many other diseases. In 2006, a systematic review of historical accounts of 37 presidents from 1776 to 1974 found that 10, or 27%, had evidence of a psychiatric disorder while in office.
Yet there is no direct correlation between a leader’s health and performance in office. Many historians give a healthy President Carter (who is now age 99) low marks for performance. President Franklin D. Roosevelt was paralyzed by polio at age 39 in 1921 and died of a stroke at age 63 after experiencing high blood pressure and coronary artery disease for years. Still, Roosevelt is judged as one of America’s greatest presidents.
That’s because age is more a physiological state of health than a chronological number — a state that can be difficult to measure and is open to varying interpretations; people grow old in different ways at different times in various patterns, making chronological and physiological ages distinct entities. Because candidates rarely release actual medical records, I have learned that the most reliable way to evaluate who is up for the physical and mental demands of the White House is through extensive interviews with the candidates and their doctors. Short of that information, it’s left to the candidates to convince voters they are fit to serve a full term.
Polls have shown that many voters wish for younger candidates to face each other in the 2024 general presidential election. Voters perceive candidate health in differing ways. Many accept at face value the medical assessments from doctors who have examined the candidates. Others form opinions based on news reports and visual sightings on television and social media, or draw on personal experiences with aging family and friends.
Both Trump and Biden have released recent information from their current doctors attesting to their good medical condition: Biden made public a detailed summary of his last physical examination, in 2023, by a team of doctors at Bethesda. In late 2023, Trump released a single-page note from his current doctor that had very few details, though he did share a White House report of a multi-doctor team examination at Bethesda in 2017.
Medical experts have urged a greater role for cognitive screening tests in evaluating the health of candidates. Trump boasts about acing the Montreal Cognitive Assessment during that 2017 exam. But he has not reported whether his current doctor has repeated a similar test; if so, when; and the result. Furthermore, neither candidate has made his doctors available to journalists for probing interviews.
Both men have shown changes associated with age since their first face-off in 2020, including erring in naming domestic and foreign leaders and various countries. Such mix-ups are common and embarrassing among those who speak off the cuff, but their significance in evaluating a candidate’s health is uncertain.
A recent news cycle has shown the limits of not having reliable medical information to evaluate presidential health. Special counsel Robert K. Hur caused a political ruckus by characterizing Biden as a “well-meaning, elderly man with a poor memory” who had “diminished faculties in advancing age” in a report explaining why he would not be charged concerning misuse of classified information.
But Hur is a lawyer, not a doctor with expertise in evaluating cognitive function decline. His assessment was based on contact with Biden for five hours and 10 minutes over two days. In his opinion, “it would be difficult to convict” Biden “of a serious felony that requires a mental state of willfulness.” Neither a transcript nor a video recording of Hur’s session with Biden has been released publicly.
Without that material, it is impossible to say how valid Hur’s assessment is. The manner, tone, and expressions of speech can be valuable clues in assessing cognition.
To truly evaluate our candidates’ fitness for office, we need more than a special prosecutor’s reports and clips of brief trouble with recall. It is only prudent for leaders and their doctors to be fully transparent in disclosing a leader’s health information because the public has a right to know it. Too often, the public has learned belatedly that candidates and their doctors were not forthcoming in disclosing their health information. In fact, a few have distorted the facts, if not lied.
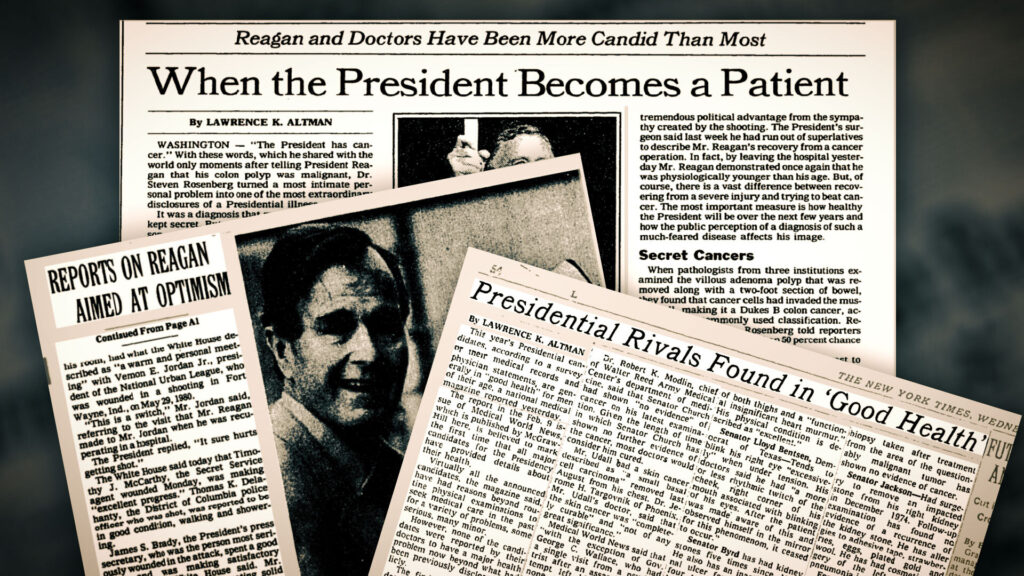
Almost six years after leaving office, Reagan announced that he had received a diagnosis of Alzheimer’s disease, inviting questions whether, in retrospect, the disease had affected Reagan’s performance in office.
Reagan’s White House doctors, who saw him daily and examined him periodically, repeatedly said they never detected symptoms of dementia during his two terms. Even so, the timing of the dementia issue remains unresolved in large part because Reagan’s medical records, like those of other presidents, are not available for analysis by independent medical experts.

After Reagan, Americans elected four younger presidents — George H.W. Bush (64 when he took office), Bill Clinton (46), George W. Bush (54), and Barack Obama (47). They were fairly representative of the age range of most presidents, who until Reagan took office were in their 40s, 50s, or 60s.
In 1996, Clinton’s opponent, Bob Dole, agreed to an interview and gave permission for me to talk to his doctor because he wanted the public to know that despite well-known medical issues he was healthy “except for some physical things.” Dole was 73 at the time and would have been the oldest president. He had wounds suffered while an infantry officer in Italy in World War II, injuries that had made him the most severely handicapped nominee for president. Dole was quadriplegic for more than a year from the war wounds. He slowly recovered the use of his legs and left arm, but his right arm was nearly useless. Also, he lost a kidney; the remaining one compensated by growing larger. In 1991, Dole had surgery to remove a cancerous prostate gland; tests showed no evidence of recurrence.
Despite all that, Dole dealt with the age issue by saying he did “not forget many things” and exercised his memory to keep it sharp by thinking about Senate affairs.
Dole lost, of course, but in recent years the age pendulum has swung back to older leaders. In 2016, Trump at 70 defeated Hillary Clinton, 69.
For all the attention to age, anyone can experience ill health at any age. An indisputable fact is that risks of developing many ailments increase with advancing age. A particular concern is the incidence of Alzheimer’s and other forms of dementia among older people. Studies have shown that 17% of Americans aged 75 to 84 years and 32% of those 85 or older have dementia.
But that means more than two-thirds do not have dementia.
It would behoove voters and political journalists to keep that in mind.
Lawrence K. Altman is a physician, a clinical professor of medicine at New York University, and former reporter and “The Doctor’s World” columnist for the New York Times. He is researching and writing a book on the health of political leaders.